In 2003, UCLA epidemiologist James Enstrom and I published a study of environmental tobacco smoke (ETS)—also called "secondhand smoke" or "passive smoking"—in the British Medical Journal (BMJ). Using data from the American Cancer Society's prospective study of 1 million adults, we concluded that ETS exposure was not associated with increased mortality.
Since that conclusion flew in the face of the conventional wisdom that had long driven state and local bans on smoking in public places, our study understandably sparked a controversy in the public health community. But the intensity of the attack on us in the pages of a medical journal—by critics who were certain that our study had to be wrong but typically failed to provide specific evidence of fatal errors—vividly illustrates what can happen when policy preferences that have taken on the status of doctrine override rational scientific debate.
A recent study by American Cancer Society (ACS) researchers underscores that point by showing that, contrary to what our critics asserted, the cancer risk posed by ETS is likely negligible. The authors present that striking result without remarking on it, which may reflect their reluctance to revisit a debate that anti-smoking activists and public health officials wrongly view as long settled.
Exposure to ETS is known to cause eye and throat irritation and to exacerbate preexisting respiratory conditions. In addition, it is simply disagreeable to many people (including me). But assessing the claim that ETS is potentially deadly requires dispassionate examination of the available scientific evidence.
That is not what Enstrom and I encountered when we published our BMJ paper. Critics were outraged by the article and demanded its retraction. But they were never able to satisfactorily explain why such an extreme step was justified.
Our Study
We addressed the main criticisms of our paper in a detailed authors' response. The journal's editor in chief defended the decision to publish the paper, enumerating its strengths and stating that failure to publish high-quality work distorts the scientific record. If anyone had found evidence of fraud or even serious errors in the paper, as some alleged, it would have been retracted. No one found any such fatal flaws.
Because we were aware of the difficulties in measuring secondhand smoke exposure, we went to great lengths to obtain fine-grained information from the California participants in the original ACS study of 1 million Americans, which was launched in 1959. We recontacted surviving members of the cohort and asked them additional questions about their exposure to cigarette smoke. Using data from multiple contacts with subjects, we were able to improve the quality of exposure information, which is the Achilles heel of most ETS studies. As a result of these measures, exposure information was more detailed and more reliable than in many previous studies.
To put the risk from secondhand smoke in perspective, we examined the association of active smoking with mortality from lung cancer, coronary heart disease, and chronic obstructive lung disease. We demonstrated dose-related associations of smoking with mortality in all three categories. This was true even for "light" smokers—people who smoked fewer than 10 cigarettes per day. That finding was important because it showed that our study was able to pick up the relatively small effect of light smoking.
The fact that we demonstrated a strong association between active smoking and mortality, which increased in a graded fashion with increasing levels of smoking in both men and women, provided consistent and impressive support for the effects of active smoking. In contrast, our results for ETS exposure showed no significant association with mortality.
The response to our paper was largely political. This was evident from the fact that the ACS attacked the paper during the two-day embargo period, before it went online. The clear intent was to delegitimize the study in the court of public opinion. This initial attack invited others to pile on, alleging flaws in our methods. But as the BMJ's editors pointed out, those charges generally were not backed by any reference to actual data from the paper.
The head epidemiologist at the ACS condemned our paper as tobacco industry "disinformation," and other tobacco control activists went even further, citing our paper in a federal racketeering case against cigarette companies. They alleged that the paper was part of a tobacco industry conspiracy to discredit scientific evidence concerning the hazards of smoking. This use of lawfare rather than open scientific debate seemed designed to have a chilling effect on researchers studying passive smoking, discouraging them from reporting politically inconvenient results.
The organizers of this attack felt it necessary to portray us as corrupt agents of the tobacco industry, even though we had long track records researching the effects of smoking and other questions in public health. Our paper included a 200-word declaration stating that the tobacco industry had no involvement with the paper.
This is not the way scientific papers typically are reviewed by "experts in the field." We thought we were publishing a scientifically straightforward, even boring, paper that presented a well-supported case. In our long careers publishing on a wide variety of topics in epidemiology, we had never run into anything like the uproar created by our BMJ article.
Despite vigorous defenses of the paper, its status became ambiguous. On one hand, it had been publicly trashed. On the other hand, it had been published in a leading medical journal and was cited in the medical literature together with other studies that showed similarly weak and uncertain results concerning the effects of passive smoking.
The New ACS Study
The new paper from the American Cancer Society, published last April in CA: A Cancer Journal for Clinicians, comes 21 years after the brouhaha over our BMJ paper and sheds further light on the controversy. This major ACS paper aims to further reduce the incidence of cancer by providing data that can be used to improve policies and practices.
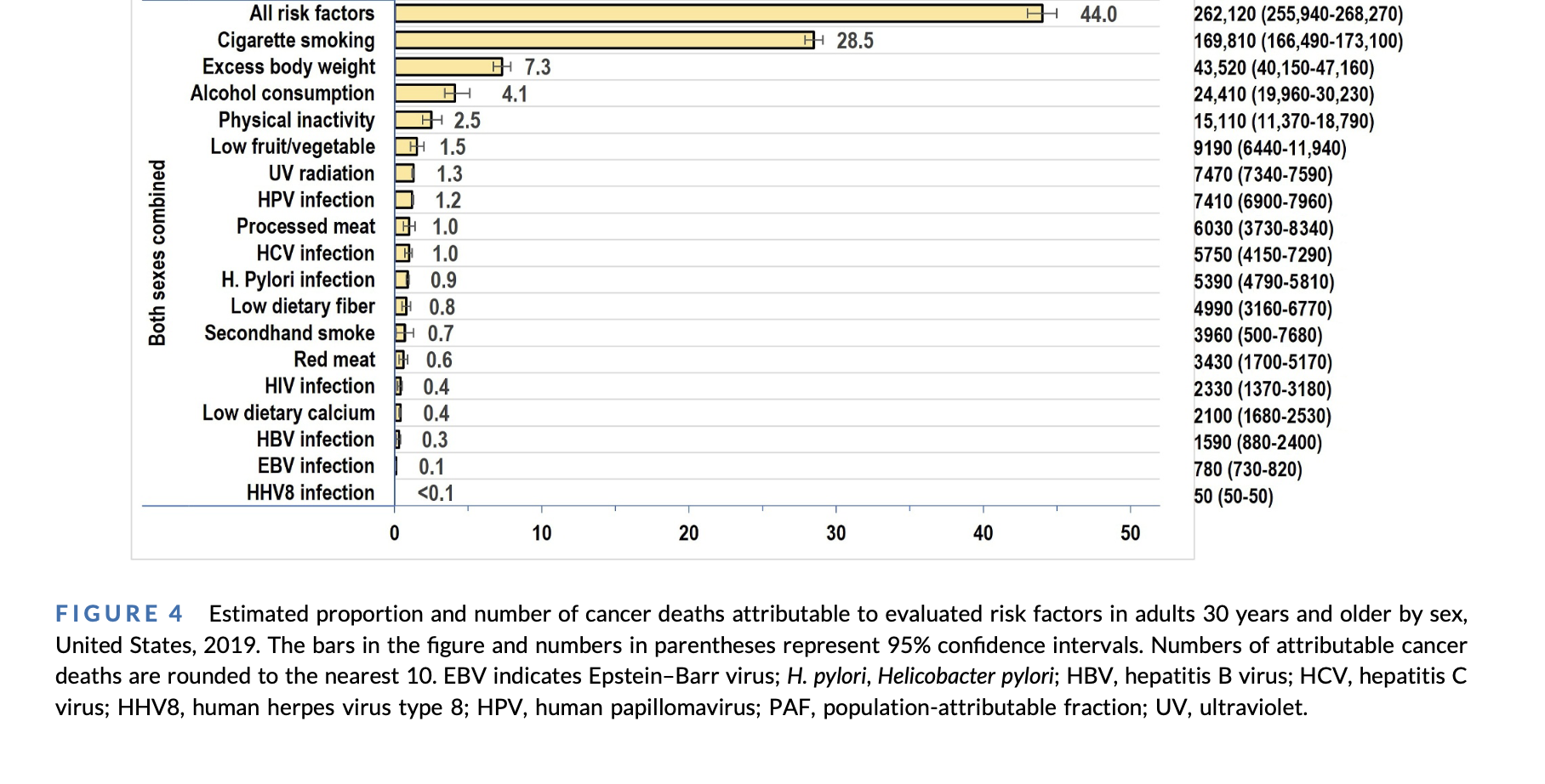
Based on U.S. risk factor data from 2014, the paper estimates the number and proportion of cancers attributable to potentially modifiable factors that the authors deemed, based on the literature, to be significantly associated with cancer risk. Cigarette smoking is by far the leading risk factor, accounting for 20 percent of all cancers and 30 percent of cancer deaths. (See Figure 4, bottom panel: both sexes combined.) The next strongest, but far weaker, risk factor is excessive body weight, followed by alcohol consumption, physical inactivity, low fruit/vegetable intake, UV radiation, HPV infection, processed meat consumption, HCV infection, H. pylori infection, low dietary fiber, and secondhand smoke, which ranks 12th.
The "population-attributable fraction" (PAF)—that is, the share of cancer deaths that could be prevented if a given risk factor were removed—is 28.5 percent for cigarette smoking and 0.7 percent for secondhand smoke—a 41-fold difference. Although the PAF for secondhand smoke is statistically significant, the magnitude of the risk is negligible and similar to the risk estimate in our BMJ paper.
A relative risk of 1.0 denotes "no increased risk." In our study, the lung cancer risk for never-smokers married to ever-smokers, compared to the risk for never-smokers married to never-smokers, was 0.75, and the difference was not statistically significant, indicating no elevated risk from ETS exposure.
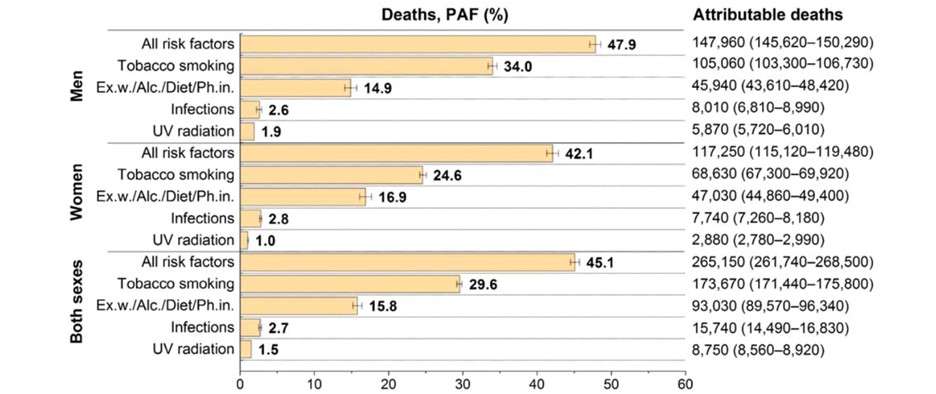
Having put the cancer risk from secondhand smoke in the proper perspective relative to the risk from smoking, the CA study combines the two exposures to obtain the total number of cancer cases and cancer deaths attributable to "tobacco smoking." The reasoning here is that if smoking were eliminated, secondhand smoke exposure also would be eliminated. But it's notable that cancer deaths attributed to ETS account for just 2 percent of the total.
The CA paper, which used survey data regarding health behaviors and national statistics on cancer incidence and cancer death rates, took a different approach from our BMJ paper, which used a prospective study of a defined population. The results of the two studies nevertheless are strikingly similar. In both studies, we see a strong risk of fatal disease associated with smoking, in contrast with a small-to-negligible risk associated with exposure to secondhand smoke.
The CA study was limited to cancer. But our results regarding ETS and coronary heart disease were particularly important, because heart disease is much more common than lung cancer and accounts for more smoking-related deaths. As we showed in our analysis, the risk of heart disease death among smokers is markedly smaller than the risk of lung cancer death. We nevertheless observed statistically significant, dose-related increases in heart disease mortality among male and female smokers. In contrast, the relative risk associated with ETS exposure was 0.94—which, again, was statistically indistinguishable from a relative risk of 1.0, indicating no increased risk.
Understanding Small and Uncertain Risks
Humans are not good at conceptualizing the very large or the very small. Think of the billions of galaxies composed of trillions of stars or the size of an atomic nucleus. When it comes to evaluating potential hazards like passive smoking, we need to realize just how small and uncertain the risk suggested by these two studies is, which is consistent with the risk found by all studies of the question.
What do I mean by a "small-to-negligible risk"? Meta-analyses combining studies of secondhand smoke exposure and risk of lung cancer in people who never smoked have reported increases in different population groups: 24 percent in studies from the U.S., Europe, and Asia; 21 percent for Western industrialized countries; and 15 percent in studies restricted to North America. Such increases are very small in epidemiology. For comparison, the elevated risk of lung cancer among current smokers is on the order of 1,000 percent, while the risk increase for heavy smokers is around 3,000 percent.
When we are dealing with risks of this very small magnitude and exposure information of uncertain quality, we cannot rule out confounding or bias even in the best epidemiologic studies. And given the likelihood of publication bias, which favors positive results, the cancer risk from passive smoking may in fact be zero.
Although the borderline results of epidemiologic studies linking secondhand smoke exposure to increased risk of lung cancer have been interpreted as providing definitive evidence of an association, more rigorous studies have received much less attention. Two careful studies carried out in the 1990s—one in the U.S. conducted at the Oak Ridge National Laboratory, the other in the U.K. by Covance Laboratories—measured actual ETS exposure of nonsmoking subjects at home and at work.
In these studies, participants wore monitors that took samples of the air in the subject's "breathing zone" over a 24-hour period. One monitor was used during daytime activities, and a second monitor was placed by the bed during sleep hours. For people living with a smoker, the home was the greatest source of ETS exposure. The average dose of particulate matter inhaled by a nonsmoker exposed to other people's cigarette smoke was equivalent to smoking about eight to 10 cigarettes per year. By comparison, the intake of the average pack-a-day cigarette smoker is 7,300 cigarettes per year—about three orders of magnitude greater.
It is striking that these careful measurement studies are rarely cited in the epidemiologic literature on ETS, presumably because doing so would weaken the case that ETS poses a major threat. Yet studies that directly measure ETS exposure represent a higher order of evidence than epidemiologic studies, avoiding the pitfalls of examining the association between an exposure proxy and a clinical outcome (e.g., lung cancer). In the latter situation, there is a danger that researchers, believing their hypothesis and aware of the consensus on ETS, will select results from their data that support an association, choosing among different comparisons based on different measures of exposure.
Researchers could, for example, simply compare exposed vs. nonexposed groups, or they could take into account the number of family members who smoked, years of marriage to a smoker, or the level of a spouse's smoking. In deciding which results to present, researchers understand that a study finding an association is more likely to be published than a study finding no association. In a study that directly measures ETS exposure, this kind of confirmation bias is less likely.
Overlooked Weaknesses
Looking at the passive smoking story from 30,000 feet, we can see that scientists reported these very small risk estimates as grounds for mortal fear. In their eagerness to publicize their findings, researchers did not examine the weak data on ETS in light of the basic methodological considerations they teach their graduate students, such as the distinction between correlation and causation, possible misclassification of exposure, confounding variables, publication bias, and other potential biases. The news media, public health authorities, and the scientific community all followed suit, deeming the evidence strong. Anyone who questioned this dogma was branded a shill of the tobacco industry.
In my 2008 book Hyping Health Risks, I explored this kind of distortion and exaggeration of uncertain or very small risks, a phenomenon that manifested itself in connection with a wide variety of potential health hazards. To guard against that tendency, it is important to compare the magnitude of a novel risk to that of other risks we know more about. In the case of secondhand smoke, it was crucial to compare the small and uncertain effects of ETS exposure to the more substantial and better studied risks associated with smoking.
When you do that, you can see that our risk estimates were not out of line with those of other studies, notwithstanding the emotionally charged and politically fueled reaction to our paper. We had merely interpreted our results—and the totality of results on this question—as implying that the risk of fatal disease from secondhand smoke exposure "may be considerably weaker than generally believed."
For the scientific enterprise to succeed, unpopular findings must be discussed objectively, rather than dismissed summarily as obviously wrong. Leveling ad hominem attacks at researchers for alleged pro-industry bias is no substitute for a rigorous and fair-minded analysis of the data.
The post We Were Wrong To Panic About Secondhand Smoke appeared first on Reason.com.