
Five million children under five years old died in 2021. Of these, nearly half occurred within the first month – a time of high vulnerability. Sub-Saharan Africa had the highest death rate in the world: 27 in 1,000 newborn babies (1,067,000). This is 11 times higher than in countries with the lowest rates (2 deaths in 1,000), such as Australia and New Zealand.
Over the past decades, newborn mortality has been markedly lower in urban compared to rural settings in sub-Saharan Africa. This “urban advantage” has been linked to better socioeconomic and living conditions, higher literacy among women and better access to healthcare services.
In Tanzania, however, the newborn mortality rate was similar for urban and rural areas for almost two decades (1991 to 2015). Then, in 2016, a national household survey found that newborn babies in urban areas were dying at a higher rate than in rural areas.
This prompted a number of questions, which our work sought to answer. Was this true and, if so, which factors related to living in urban areas might be contributing to it? Given the rapid expansion of the urban population – particularly informal settlements – had urban areas become “the new rural” in terms of the vulnerability of newborns?
The answers are important because of the rapid ongoing urbanisation in Africa. The population is expected to nearly triple by 2050, reaching 1.5 billion urban dwellers.
Our results were clear. Babies faced a higher risk of dying in more urbanised areas. What’s more, our research points to the fact that urban populations are diverse, and certain neighbourhoods or subgroups may be disproportionately affected by poor birth outcomes. Health policies must be designed to capture this reality.
First things first
Our first task was to describe and demarcate what “urban” and “rural” really meant.
In the 2016 national household survey, the distinctions between rural and urban were made from historical and administrative boundaries. This may no longer reflect the lived reality since the boundaries do not correspond to the physical space where interactions between economic and social activities happen. With the advantage of satellite imagery, we could more precisely identify lived environments, including population, land use and cover, and extent of built-up areas.
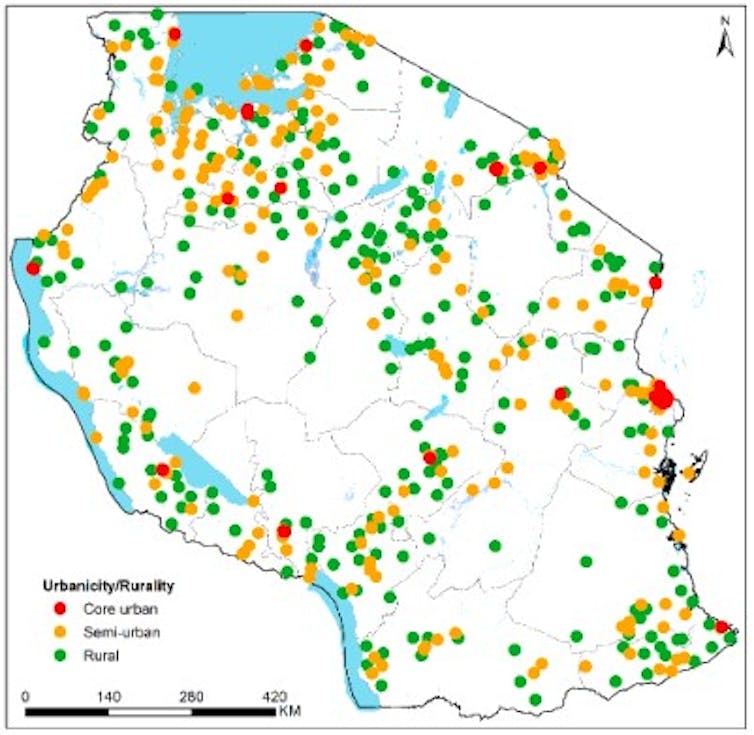
Based on these inputs and statistical methods, we categorised mainland Tanzania into three lived environments: rural, semi-urban (outskirts and suburbs of cities and towns) and core urban (densely populated inner cities) (Figure 1).
Our second task was to reflect on what newborn mortality really meant. We know that complications during childbirth are among the most important causes of death among newborns. The same complications (for example, being premature or small) and poor quality of childbirth care also lead to deaths of babies in the womb (before they are born or in the process of being born), leading to stillbirths.
We included stillbirths in addition to newborn deaths in our analysis, a combined group of deaths which is called perinatal mortality. Both help us understand the reasons babies might be more likely to die in this critical period in urban settings – whether the death occurs in the process of being born or shortly afterwards.
Mortality
For every 1,000 pregnancies, 36 babies died in rural areas, 38 in semi-urban and 56 in core urban areas.
We found similar results when we looked only at newborn mortality (babies born alive). For every 1,000 live births, 22 newborn babies died in the first month of life in rural areas, 25 in semi-urban areas and 40 in core urban areas.
Previous research has shown that the leading causes of newborn deaths are prematurity, low birth weight, birth asphyxia and infectious diseases. These are mainly related to the quality of care during pregnancy, labour and childbirth – for example, whether the child was born in a facility and in the presence of a skilled birth attendant.
But explaining why proved harder. Based on previous research – work which does not classify the urban areas as we did – it’s likely to be a combination of factors related to informal settlements in urban areas with limited access to clean water and sanitation, poor quality of healthcare, and traffic congestion limiting timely access to care for pregnant women and their babies. Poor air quality can also lead to babies being born prematurely.
Nevertheless, the reversal is not fully understood. Our findings could not be fully explained by factors such as poverty, maternal education, or the travel time to hospitals where childbirth and newborn care are provided.
However, certain factors were found to be associated with the risk of neonatal or perinatal deaths. These factors include the mother having low iron levels during the survey (maternal anaemia), a household with fewer members, having the baby being born as a twin or triplet, having a male child, a first-time pregnancy or a short time interval between pregnancies, and giving birth to a baby with either a low or a high birth weight.
Next steps
About a third of Tanzania’s population of 62 million live in an urban area. A focus on the issues relevant to urban areas is now more critical than ever if the country wants to increase the number of children who survive beyond one month.
Policy areas for action should include:
Urbanisation: policies to address the expansion of urban informal settlements are a place to start. For example, in Dar es Salaam, an estimated 80% of the land or settlements is informal. This might hamper the quality of care provided for the reasons outlined quite apart from poor sanitation practices.
Differences in urban settings: our findings suggest that policymakers must resist the temptation to lump together urban areas because this will mask the high variation within them. Unmasking variation and inequalities will aid targeted interventions.
From this starting point, policymakers can then draw lessons from existing projects found to improve urban maternal and perinatal health. These include the maternal and neonatal project at multiple facilities in Dar es Salaam to uplift the level of care at childbirth.
The project resulted in the decongestion of overcrowded hospitals, an increase in quality of care and inter-facility referral, and a reduced number of maternal deaths and stillbirths.
A similar multi-partner approach has been successful in Kampala, Uganda, as well as Rotterdam, the Netherlands, in addressing other key determinants of urban health, such as housing, social protection, income, air pollution and vulnerability to extreme climate events.
Peter Macharia was supported by the Institute of Tropical Medicine’s EWI People Program. He acknowledges the Royal Society Newton International Fellowship (NIF/R1/201418) and the Wellcome Trust support to the Kenya Major Overseas Programme (#203077).
Lenka Benova received funding from the Research Foundation – Flanders (Fonds Wetenschappelijk Onderzoek) as part of her Senior Postdoctoral Fellowship in 2019-2022 (award number 1234820N).
Andrea Barnabas Pembe and Claudia Hanson do not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and have disclosed no relevant affiliations beyond their academic appointment.
This article was originally published on The Conversation. Read the original article.







